

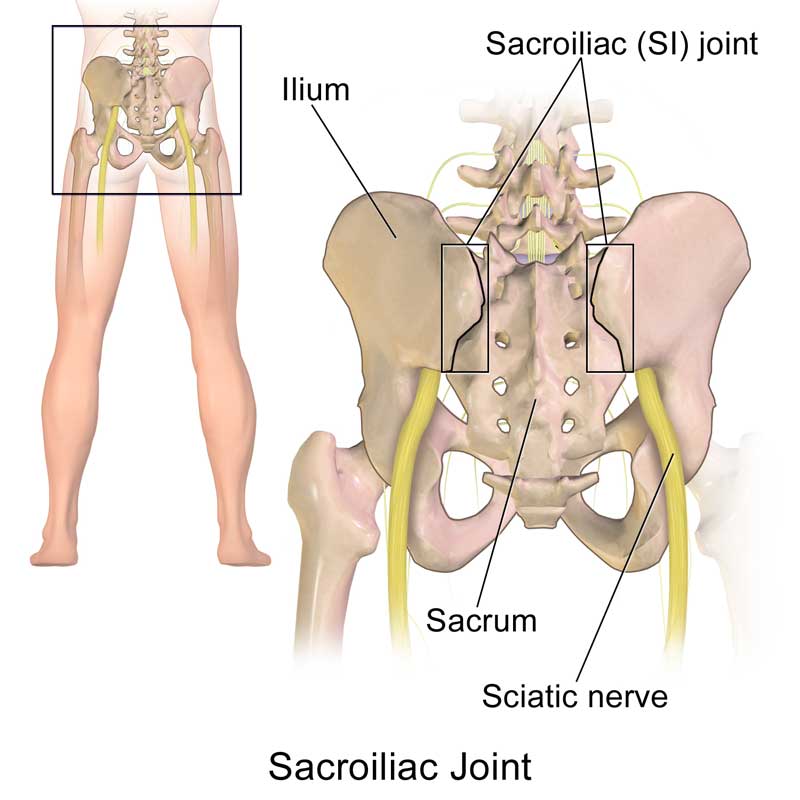
What is the Sacroiliac Joint and what does it do?

Related Articles
- Sacroiliac Joint Injections
- Sacroiliac (SI) Joint Injections (Steroid)
- Intra-Articular Sacroiliac Joint Injections (SI)
- Lateral Branch Blocks
- Articles – Back Pain (Upper & Lower)
Sacroiliac (SI) Joint Pain
Sacroiliac (SI) joint pain or dysfunction is typically caused by trauma or degeneration. Pain may be felt in the low back, buttocks, groin, tailbone as well as in the leg that can mimic sciaticasymptoms. Too much movement (hypermobility or instability) can cause the pelvis to feel unstable and lead to pain. Pain from too much motion is typically felt in the lower back and/or hip and may radiate to the groin. Too little movement (hypomobility or fixation) may cause muscle tension and pain typically felt on one side of the low back or buttocks and can radiate down the back of the leg.
People with SI joint pain often have difficulty sitting for long periods, going from sitting to standing, and sleeping. Inflammation of the joint can also cause pelvic pain and stiffness and be caused by infection, rheumatologic conditions or other causes. SI joint dysfunction is more common in young and middle-aged women especially those that are pregnant or recently given birth. Those that have had a spinal fusion of their lumbar spine are also at increased risk for possible SI joint pain or dysfunction.
Diagnosing SI Joint pain
Treating SI Joint pain
Options for treatment range from conservative to surgical, but most patients can be managed with nonsurgical treatment. In early stages, brief periods of rest, application of ice or heat, and oral medications such as acetaminophen or NSAIDs can help reduce pain, inflammation or spasms. Manual manipulation (by a chiropractor or specially trained therapist) can help if pain is caused by hypomobility of the SI joint. Bracing may help stabilize a hypermobile joint. SI joint injections can be performed not just for diagnostic, but also therapeutic purposes with the use of corticosteroids to reduce pain and inflammation.
Refractory cases that don’t respond to the usual conservative measures may be a candidate for other treatment options. Radiofrequency ablation of the sacral lateral branch nerves has shown temporary improvement and modest pain reduction at one year post treatment. Regenerative therapies, including Platelet Rich Plasma (PRP) or other autologous injections may be helpful for chronic SI joint pain. Studies have shown steroid injections may be effective in the short term (up to 4 weeks but decreased by 3 months) where PRP showed more benefit than steroid at both 6 weeks and 3 months post injection. Other studies showed ongoing relief of intra-articular PRP injection at 1- and 4-years post injection.
Surgical fusion of the SI joint is also available. If pain persists greater than 6 months and nonsurgical interventions fail (physical therapy, medications, injections), minimally invasive SI joint fusion techniques have proven to be beneficial in terms of pain relief and functional improvement. Minimally invasive fusion of the SI joint has been performed with several types of implants, including triangular, porous, titanium coated implants, hollow modular screws, titanium cages, and allograft dowels. Evidence has shown the triangular titanium implants (also known as iFuse) to provide favorable outcomes with lower complication rates at one year, and sustained long term improvement(up to 5 years).
If you suffer from low back pain, contact NERA Spine and Pain Medicine at 610-954-9400. Get Back to Life without a Surgical Knife.
Resources
- https://www.spine-health.com/conditions/sacroiliac-joint-dysfunction/sacroiliac-joint-dysfunction-si-joint-pain
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2582421/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7208275/
- https://pubmed.ncbi.nlm.nih.gov/27677100/
- https://pubmed.ncbi.nlm.nih.gov/27392848/
- https://www.isass.org/isass-policy-statement-minimally-invasive-sacroiliac-joint-fusion-july-2016/